Teach-back and behavioural communication improved self-isolation while awaiting COVID clinic test results
Self-isolation after COVID PCR testing was an essential part of the public health strategy but uncertainty around self-isolation rules was hampering compliance. Simple behavioural interventions were able to dramatically decrease self-reported breaches of self-isolation in 2020.
Key information
- The challenge: To limit the spread of Covid, self-isolation between getting tested at a clinic and getting the test result was critical. Uncertainty about when and how to self-isolate was hampering some compliance in 2020.
- What we did: In 2020, we worked with NSW Health, SydPath and Western Sydney Local Health District to run a trial to identify and remove behavioural barriers to correct self-isolation.
- Result: Our succinct handout, and 'teach-back' instructions delivered by clinicians, decreased self-reported self-isolation breaches by 29 per cent.

The challenge
During 2020 and 2021, self-isolation after COVID testing was an essential part of the public health strategy to prevent further community outbreaks of COVID. However, self-isolation behaviour confused some people. Despite good intentions, maintaining self-isolation could be challenging. People getting COVID tests may not have considered practical issues like picking up children from school, attending work, grocery shopping or visiting family. Additionally, some people who do not have severe symptoms get tested for peace of mind, or to satisfy work and childcare requirements. They may perceive lower likelihood that they are COVID-19 positive. They are subsequently caught off guard when they’re told they need to self-isolate until they get a negative test result.
What we did
We conducted fieldwork in Western Sydney to understand the behavioural barriers impacting on correct self-isolation behaviour. We found that:
- Different information materials were being used in different testing clinics. Some clinics gave customers numerous leaflets with dense information, while others may not specifically provide written instructions on self-isolation.
- Verbal briefing of self-isolation varied, with some clinics spending around five minutes to explain the importance of self-isolation in detail, while others presume familiarity and place less emphasis on self-isolation.
- There was inconsistent explanation of self-isolation behaviours. The relevant Public Health Order at the time required that people go straight home after a test, until they receive a negative test result. However, some customers would stop off along the way, or continue with their activities for the day.
Our trial began with a one-week benchmarking period (12 November to 22 November 2020), where customers were sent an English language survey prior to the intervention, to gauge a baseline of compliance.
We then delivered the intervention over six weeks, from 24 November 2020 to 3 January 2021. Everyone who was tested in nine clinics in Western Sydney Local Health District was randomly assigned to either the treatment or control group.
- Treatment: this group received a new handout and an enhanced briefing process (‘teach-back’), which were designed using behavioural insights principles.
- Control: this group received a standard NSW Health leaflet for customers with the pre-existing briefing process delivered (no teach-back).
The nine trial sites alternated between treatment and control from one week to the next, for the six-week period. The figure below provides an illustration of this process.
In addition, a further four clinics served as benchmarking sites. They were not placed into Treatment or Control. Rather, they were used to monitor the impact of testing volumes and to provide a benchmark of customer experience.
Customers who received a negative test result were invited to complete our survey about their customer service experience, as well as report on their self-isolation behaviours.
People with positive results were not surveyed for ethical reasons. People who are COVID-19 positive are under stress and already receive additional monitoring from NSW Health that reinforces self-isolation.
Almost 76,000 customers with negative COVID-19 results were sent a link to our survey via SMS. The survey could be completed in English or one of the other three biggest languages in Western Sydney, which have the lowest level of English-language proficiency: Chinese, Arabic and Korean. We received almost 8,000 valid responses to our survey across the 13 clinics. In this analysis we focus solely on responses from the 9 clinics (n=3,289), including 1,649 customers in Treatment and 1,640 in Control.
We relied on self-reported measures, including how many times customers left home while waiting for their test results. To limit social desirability bias (responding to questions in the best positive light) customers were surveyed online after they received a negative result and their required self-isolation was over, and the survey was completely anonymous. We also reduced perceived stigma by asking about a range of reasons that people may need to break self-isolation, including permissible reasons under the Public Health Order, such as seeking medical assistance.
Behaviourally informed written advice to customers
The behaviourally informed handout provided simple, but targeted, written information at the point of testing: a clear call to action, practical steps to overcome barriers to self-isolation, assurance about the 24-hour time waiting for results, and multilingual instructions.
The behavioural science techniques embedded in our handout include:
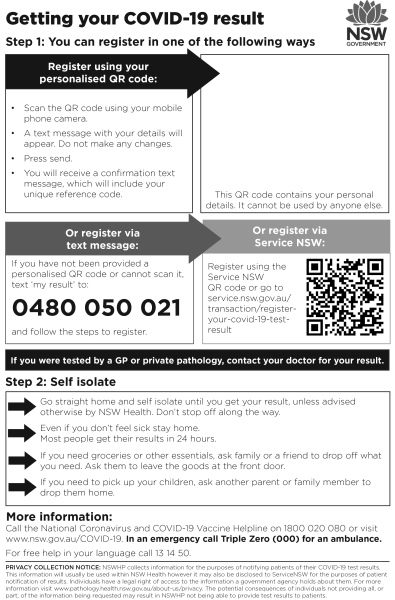
- Simplification: Breaking down complex and unfamiliar tasks into easy steps increases compliance. The handout told people the two things they need to do immediately after leaving the testing clinic: 1) Go straight home. Don’t stop off along the way. 2) Self-isolate. The instructions were provided in Easy English.
- Salience: People are more likely to pay attention to details that stimulate their senses (such as attractive colours), and which focus attention on important details. Our handout reminded people they’ll get results within 24 hours, and they should stay home even if they don’t feel sick. Graphics of the key messages aid understanding.
- Scarcity mindset: People who are busy or overwhelmed have limited ability to take in new information (PDF 142.3KB) and make optimal choices. We can help busy people who feel unprepared for self-isolation by offering suggestions to major behavioural barriers.
- Timeliness: People are more likely to take action if they receive clear directions at an optimum time. Rather than overwhelming customers with detail, we focused on essential information they need at time of testing: how to best self-isolate at home. Additional information about testing and self-isolation from the business-as-usual leaflets were accessible via a QR code. Each language had its own QR code, that led customers to a translated webpage.
- Make it easy: Asking for translated materials is sometimes a barrier. Our double-sided multilingual handout included four languages in one place. This meant customers weren’t forced to request additional help, and staff didn’t spend time trying to find the right materials for those who need it most.
A sample of our behavioural handout is included below.

Teach-back: improving what clinicians tell customers using behavioural insights
‘Teach-back’ is an effective way for health professionals to check whether customers are confident in following directions when they leave a healthcare setting. We provided clinic staff with standardised script on self-isolation that mirrors the messages in the handout. Customers were then asked to repeat back what they need to do to correctly self-isolate. Clinic staff also had a checklist, to ensure they listen for key information.
Teach-back ensures clinic staff don’t assume customers’ understanding and ability to action directions (that is, their health literacy), and provides opportunity to ask questions and clarify self-isolation issues.
The teach-back script draws on the following behavioural principles:
- Simplification: Clarifying messages strengthens compliance. The script clarifies the meaning of self-isolation and reinforces the call to action from the behavioural handout.
- Temporal discounting: People tend to discount future benefits and consequences. The script emphasises that 24 hours is a short wait for peace of mind on test results.
- Error management: People are more likely to make mistakes in stressful working conditions. Checklists present complex information clearly and concisely, ensuring important details are not missed. Our checklist ensures clinic staff can double check the customer has understood the key messages on self-isolation.
What we found
Our handout and teach-back intervention led to increased compliance. People who received our intervention were less likely to break isolation (92.5% said they never left home) compared to people who received business-as-usual service (89.5%). The difference was statistically significant.
The intervention could decrease the number of people leaving home before getting their test results by 300 people each day, or 2,100 each week for every 10,000 tests conducted. This equates to 29% fewer people breaching self-isolation weekly.
Customer satisfaction with COVID-19 clinics
The enhanced process was stress-tested during the Northern Beaches outbreak. Throughout the six-week trial period, customers gave COVID-19 testing clinics a high satisfaction rating, with an average 9.4 out of 10. Even with a significant increase in testing volume, the handout and teach-back did not impact high customer satisfaction (see the graph below).
Willingness to be re-tested
Additionally, our trial found that only 3 out of 5 customers reported they would get re-tested in less than 24 hours if they had symptoms again. This suggests continued communications could improve responses to public calls for testing.
Multilingual survey options increase response rates
We found that more people completed our survey when they received a SMS text that offered multilingual options. During benchmarking week, an average of 10.8% of people completed our survey, however, during the trial, when people had the option to complete in English, Chinese, Arabic or Korean, an average of 16.4% of people completed our survey.
Nevertheless, most people completed the survey in English. Possibly because the survey in English was simple enough for people to understand.
Our results suggest that multilingual materials boost compliance and reciprocity. Providing COVID-19 materials in multiple languages, and surveying in multiple languages, demonstrates the NSW Government is listening to multilingual communities.
Managing additional information by using a QR code
Only 11% of people used the QR code to access more information on self-isolation on the NSW Health webpages. Most people visited the English page, but spent little time reading these resources (there was a 70% bounce rate, meaning people left within seconds of opening the page).
Our results suggest that QR codes may be useful for instrumental purposes (e.g. COVID Safe check in), but less impactful in delivering health education. Further testing is required on the efficacy of QR codes for delivering complex health information. It seems likely that the public requires less information and responds well to simplified directions that clarify what they need to know on the spot.
What’s next
After reviewing the research findings, in 2021 NSW Health has:
1. Redesigned the written information provided to customers at public COVID testing clinics
- The new information provides easy-to-follow instructions, which addresses common behavioural barriers that lead to people breaking self-isolation
- The new information includes practical tips on how to plan ahead, such as asking friends to drop off groceries or for family to pick up children from school
- A personalised QR code allows customers to register for their test results following a small number of simple steps
- Translated information is available to maximise community reach.
2. Provided new training resources to all clinic staff across NSW, including a training video produced by the Health Education and Training Institute. In the first three months of use, over 1500 NSW Health staff had completed the training.
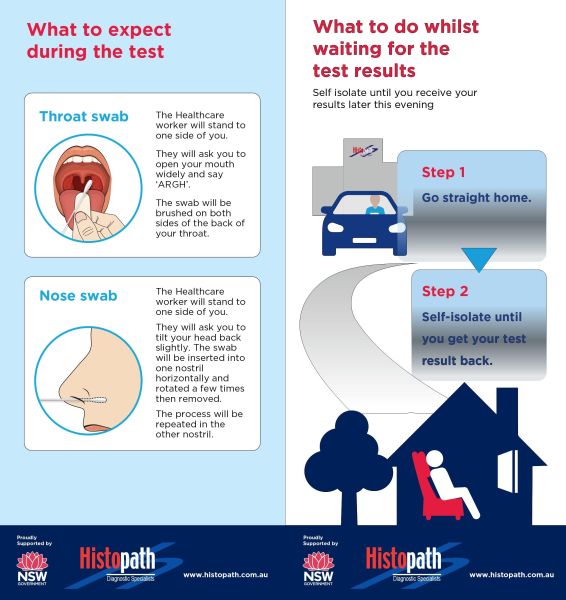
Additionally, private clinics around NSW have adopted advice on behavioural communications into their practices (see the example from Histopath below). In the first three months of implementation, there were 1,000 unique views of the webpage for private clinics containing the teach-back training.
How can you use this in your work?
Lessons from this trial can be used to improve information or other services that require behavioural change.
- Provide timely information: people are more likely to comply with a short call to action. Focus on what they need to do right away. Give customers practical advice to help them overcome barriers. Use salient features, like simple graphics and bright colours to call attention to important details.
- Provide multilingual materials and feedback: people are more likely to comply with behaviours with multilingual translations that are made easy. Rather than simply expecting customers to call translation services, or navigate webpages to find relevant information, make it easy by including the top languages in your local service area. Providing multilingual surveys also increases people’s willingness to complete a questionnaire.
- Make customer service easy: when introducing a large behavioural change for customers, provide a behavioural script for staff delivering services, so they cover important information succinctly. Include a checklist as a prompt to help staff.